OSTEOARTHRITIS SLIDES AND ANIMATIONS
©2004 All rights reserved. I would like to share my materials for educational purposes. Also, see my thoughts about other uses for my content at the bottom of the page.
This menu immediately below is for a new site using a different format for presentation. It has most of the material on the older talk below, except for the information on NSAIDs, but it has a lot more on normal joints and OA. Try it out.
Lecture #2 Osteoarthritis and the NSAID WARS - 1998
This is a talk that was given to the Idaho Academy of Primary Care Physicians on May of 1998 on Osteoarthritis and NSAIDs as a multimedia presentation. Much of this material was made for my "Overview of Rheumatology" lecture for the U.C.L.A. medical students from 1995 to 1998. Toolbook was originally used for presenting this web site. The web site contains still slides as jpegs and animations as avi files. The avi files require a broadband connection for reasonable downloading times. I have left all the original material from this site which was first posted in 1998, but I am adding material in different formats, such as quicktime (mov) files for downloading, and flash for easy of viewing.
You should download the Macromedia
Flash driver version 6 or higher to best view this site. ![]()
Craig Wiesenhutter
OSTEOARTHRITIS Slides and Animations Part 1

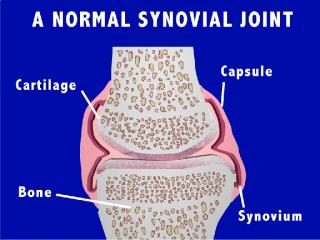

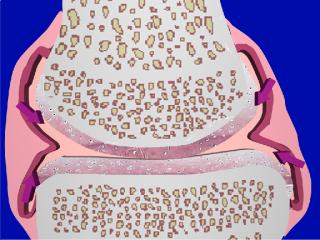
Slide #1: In transit to Sun Valley. Slide #2 presents the title of the talk as osteoarthritis (OA). The importance of osteoarthritis is discussed. It is the most common arthritis, and it is the most common chronic illness in people over 65 years of age. There have been a lot of new advances concerning pathophysiology as well as new concepts about the development of "joint failure", which will be presented. The second part of the talk will deal with NSAIDs and will focus on side effects (Slide #3). New NSAIDs, i.e., Arthrotec, and the highly selective Cox 2 agents will be discussed. Slide #4 is a schematic drawing of a synovial joint. The structure and function of the capsule, synovium, hyaline cartilage, and subchondral bone are discussed. Slide #5 is a 3D model of a normal knee joint, anterior oblique view.

In Slide #6, Joint Stability, we discuss the contribution of ligaments, the joint shape, muscle action, and synovial fluid adhesion. Slide #7 shows muscles supporting the ankle joint in a dynamic fashion. Slide #8 shows the secretion of lubricating materials from the synovial lining cells.

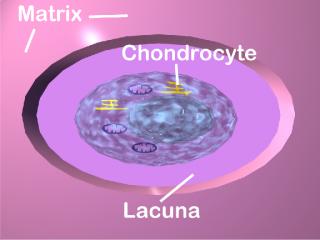
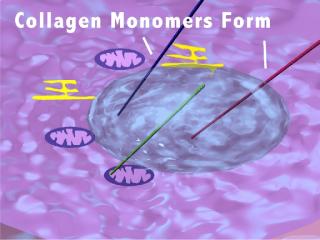
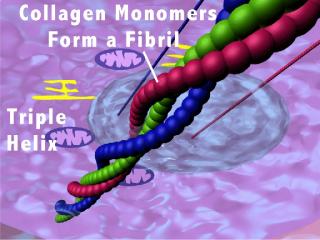
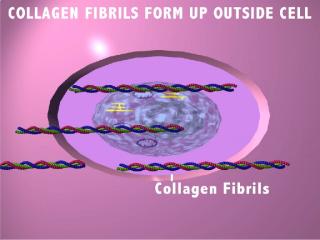
In Slide #9 we begin a close-up look at hyaline cartilage. Slide #10a shows a chondrocyte in its lacuna. The cell contains organelles for protein synthesis. The cartilage matrix surrounds the lacuna. Collagen is synthesized within the cell (Slide #10b) and 3 monomers of type II collagen form a triple helix resulting in collagen fibrils (Slide #10c). The collagen fibrils move outside the cell and form cross-links (Slide #11a-b).
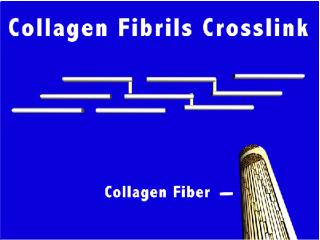
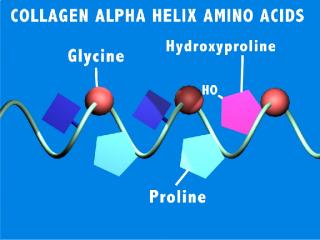
The fibrils form collagen fibers which also have cross-links between each fiber resulting in structures which have very high tensile strength. There are several different kinds of collagen (>14 so far described) which are defined by their unique series of amino acids shown in Slide #12.
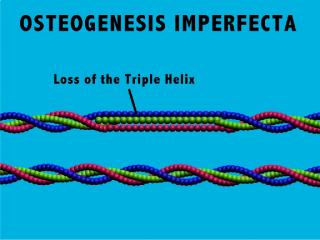

The chemical structure of these amino acids encourage the formation of the triple helix. Slide #13: Type I and type II collagen are the most important collagens in the matrix of bone and cartilage respectively. Slide # 14 depicts a disease, Osteogenesis Imperfecta in which there is a substitution of a cysteine for the glycine of the collagen helix. This genetic disease results in a dramatic abnormality in the structure of bone which leads to frequent fractures occurring at an early age (Slide #15 ).

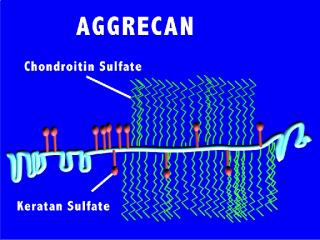
In addition to collagen, the other major constituent of the cartilage matrix is proteoglycans. The most important proteoglycan is aggrecan, which is shown in Slide #16. Aggrecan is a giant, complex macromolecule. The polysaccharide side chains are hydrophilic and attract water. They also have multiple negative charges which cause the molecules to repel each other. The aggrecan is then attached to a hyaluronate core molecule (Slide #17).
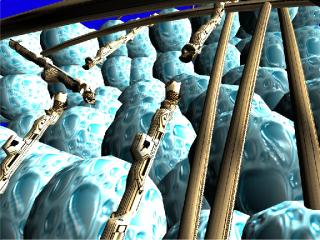
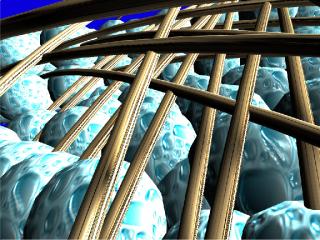
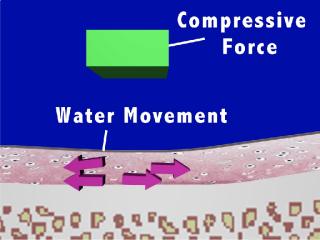
Slide #18 shows a schematic of cartilage. The collagen fibers restrain the aggrecan molecules (blue water balls) so that they can only partially absorb their maximal content of water. This leads to a tissue which is highly turgid and which has marked resilience. In Slide #19 an early change in OA is shown, and there has been damage to the collagen fibers. There is a loss of restraint on the aggrecan molecules and the molecules will expand, or be lost from the matrix, and the cartilage will lose its resilience. When there is a compressive force on the cartilage, the water within the aggrecan molecules also freely moves, as is shown in Slide #20. Water movement allows for distribution of mechanical stress. Once the force is removed,
OSTEOARTHRITIS Slides and Animations Part 2
the water returns to its previous location, ready for the next impact. Also, water makes its way to the surface of the cartilage and acts as a hydrostatic cushion, protecting the cartilage.
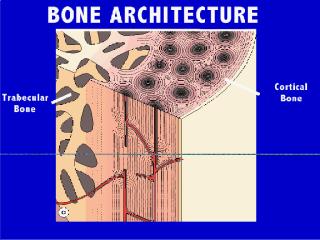
Bone is intimately associated with cartilage. Cartilage is calcified at its interface with bone, which assures a solid attachment between the two tissue.
Slide #21 shows the architecture of bone. In Slides #22 & #23 bone remodeling is described. There is constant formation and resorption of bone.
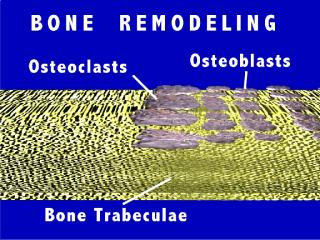
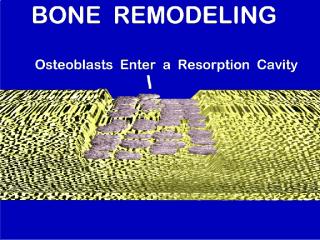
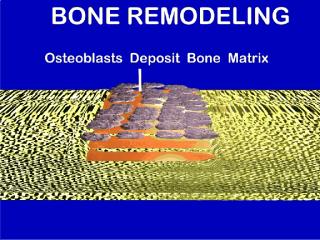
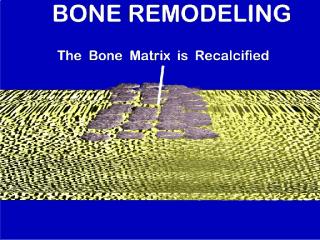
Slide #24a-d shows the remodeling sequence, which is animated in the talk. Cartilage also has a significant degree of turnover. We have discussed the production of collagen and proteoglycans by the chondrocyte.

The cartilage matrix components are metabolized by several matrix metalloproteinases (MMP’s Slide #25). MMP’s are discussed and the one of the four categories of MMP’s, i.e. Collagenases, is used as an example, and a cartoon collagenase (Slide #26) is shown preparing to split the collagen fibers (collagenase actually splits the triple helix).
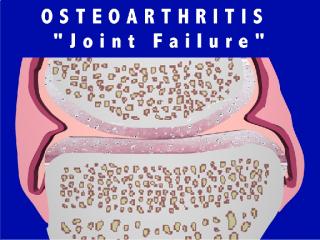
Osteoarthritis is discussed (Slide #27). The paradigm of "Joint Failure" is presented (Slide #28). Joint failure is similar to other organ failure in that there are many pathways to the same end stage. I discuss the fact that I’ve seen 3 patients within the past few weeks, all with severe knee OA. One patient is 40 y/o 300 lb. stockbroker who injured his knee playing football in highschool. His knee is his only arthritic joint. A second patient belongs to a family in which both he and his siblings and his mother has required a total knee replacements in their 30’s-40’s. Studies on similar families have shown an abnormal collagen gene in these families. A third patient seen in the clinic is a 40 y/o retired prostitute who acquired a septic knee secondary to gonorrhea as an 18 y/o. She has an end-stage knee and will require a total knee replacement in the near future. All of these patients developed "joint failure" but by different mechanisms. The knee is morphed during the talk showing the characteristic changes of OA, i.e. a loss of cartilage thickness, a ragged surface to the cartilage, new bone forming at the margins as osteophytes, and a distortion of the capsule. Debris entering the joint space is taken up by phagocytes in the synovium leading to inflammation and thickening. Inflammation does occur in OA, just not to the extent seen typically with RA.
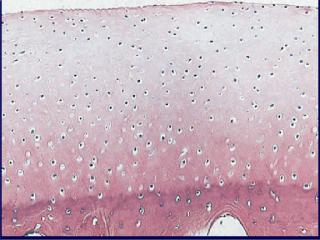

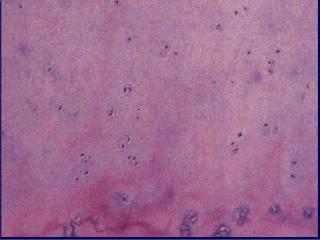
Slide #29 shows a normal histologic section of cartilage (from Dieppe Textbook of Rheumatology).Slide #30 shows abnormal cartilage in early OA where there has been a drop-out of chondrocytes secondary to necrosis (from Dieppe Textbook of Rheumatology). Slide #31 shows abnormal cartilage in which there are nests of chondrocytes forming in an attempt to repair the damage (from Dieppe Textbook of Rheumatology).
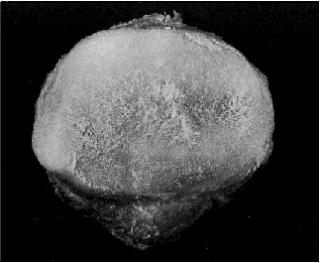
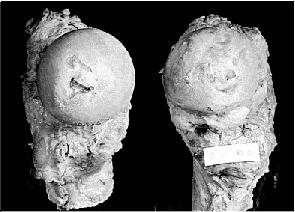

Slide #32 shows the undersurface of a patella in a patient with chondromalacia patella. This condition is most likely a precursor to OA and results in excess water in the cartilage (from Dieppe Textbook of Rheumatology). Slide #33 shows two gross specimens of femoral heads (from Dieppe Textbook of Rheumatology). The hip on the left demonstrates mild OA with some focal loss of cartilage at the center. The hip on the right demonstrates severe OA with near complete loss of cartilage and the formation of large osteophytes. Slide #34 shows the MRI scans of the specimens in Slide #33 (from Dieppe Textbook of Rheumatology).

Slide #35 shows a mother and daughter with OA of the big toe (bunions). The genetic contribution to OA is discussed. Is this because of inherited collagen, proteoglycans, ligaments, capsule, or what?
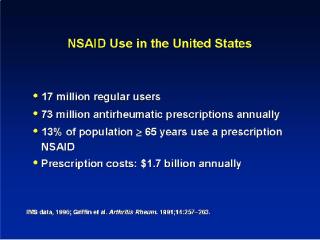
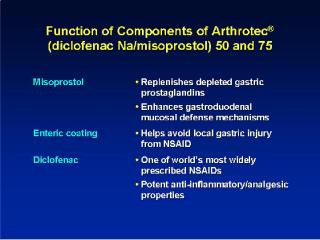
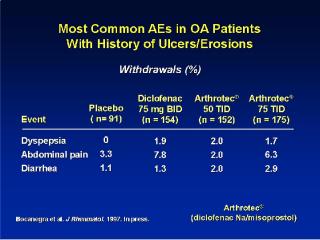
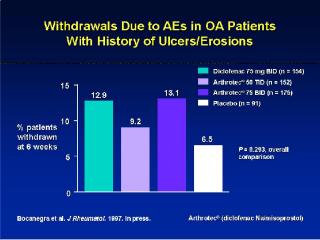
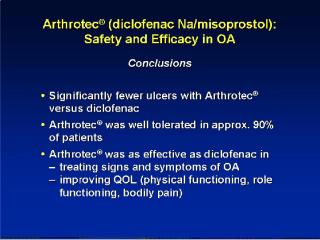
The last part of the talk covers the new NSAIDs and their complications. Several NSAIDs are competing for the huge market for prescription NSAIDs. No NSAID can claim superior efficacy. So, the final determination of which NSAID to use will come down to cost and safety.
These last 7 slides are from Searle Pharm.
OSTEOARTHRITIS Slides and Animations Part 3
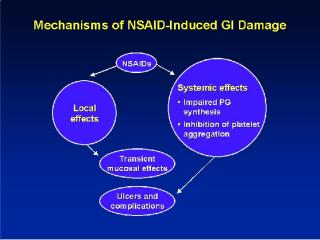
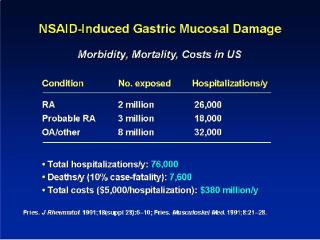
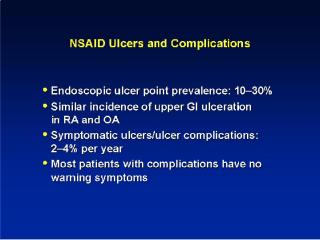
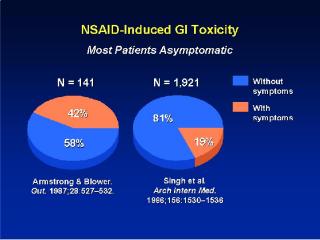
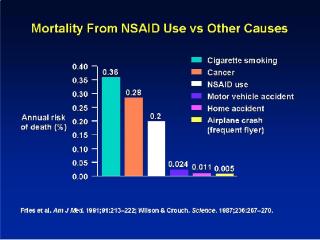
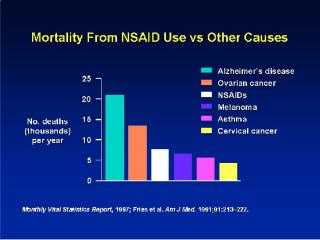
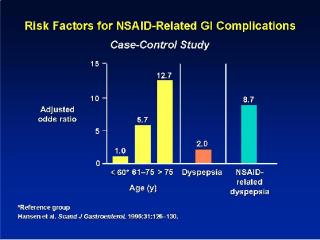
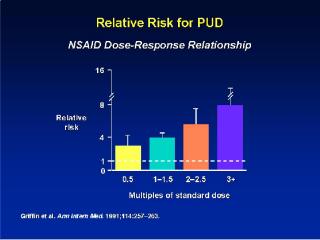
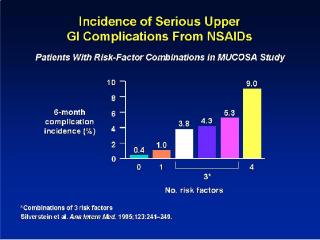
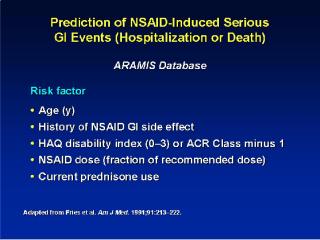
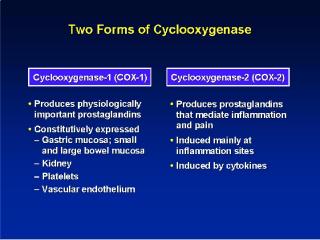
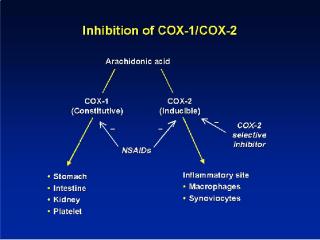
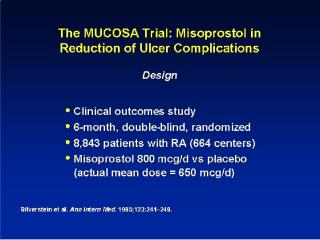
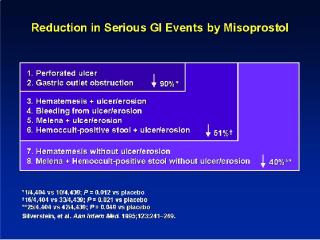
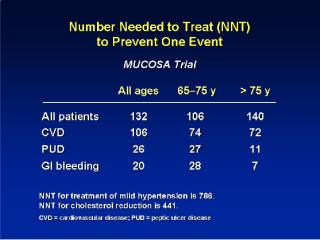

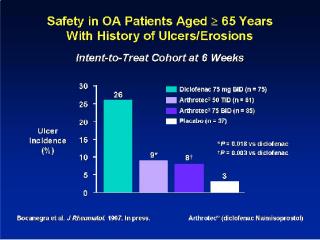
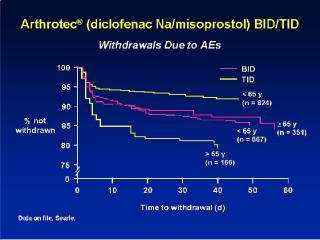
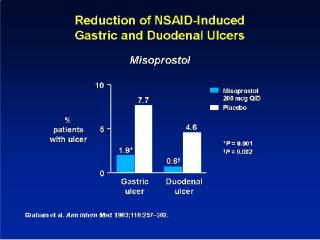
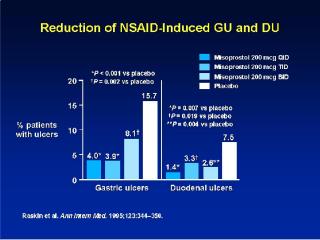


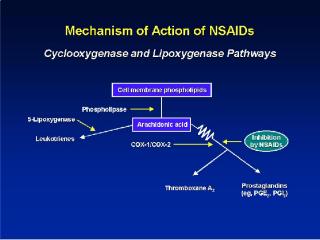
Numerous studies suggest that the incidence of clinically significant GI events is from 1-4% per year for NSAID’s. There is a debate whether certain currently marketed compounds are safer and this topic will be discussed. There are now several compounds under study that have been designed to be highly selective inhibitors of Cox 2 while sparing Cox 1. It is hoped that these agents will have far less toxicity than previous agents while still maintaining efficacy. This topic will be discussed.
 (The cox 2 slide is from the Searle Pharm. web site.
(The cox 2 slide is from the Searle Pharm. web site.
)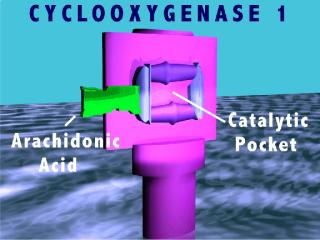
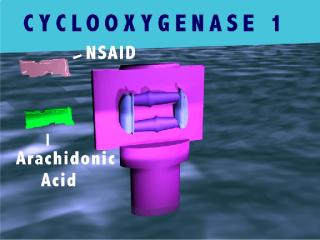

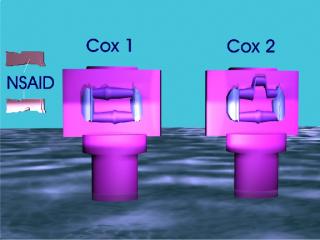
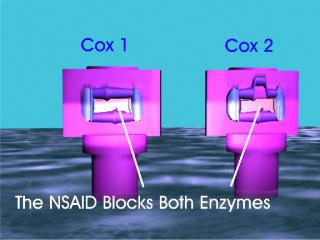
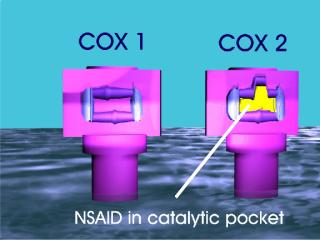
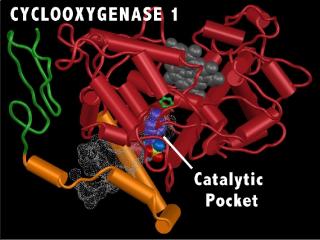
Models of Cox 1 and Cox 2 with the interaction of NSAIDs (both nonselective and Cox 2 selective) will be animated and discussed. One very promising treatment will be presented, i.e. MMP inhibition in both the treatment of RA and OA. The possibility that the deformities in RA could be significantly reduced or prevented as well as the possibility for disease modification in OA will be raised. In summary, there are now numerous new concepts about arthritis disease development as well as as variety of new treatment approaches. I expect to see several major advances in the understanding and treatment of arthritis in the next few years. It is a very exciting time for Rheumatology.
Slides, artwork and photos by Craig Wiesenhutter, M.D. unless indicated.
References:
Klippel, John H., and Paul A. Dieppe, Rheumatology, Second Edition. Mosby. This is the best textbook for this subject.Hubbard, R.C., Koepp, R.J., Yu, S., Talwalker, S., Geis, G.S., Wiesenhutter, C.W., Makarowski, W.S., and H.A. Paulus. SC-58635 (CELECOXIB) A Novel Cox-2 Selective Inhibitor, Is Effective as a Treatment for Osteoarthritis (OA) In a Short-Term Pilot Study. Arthritis Rheumatism, 1996 Sept (Suppl), 39(#9): p. S123 Abstract #574
Hawkey et all "Omeprazole compared with Misoprostol for ulcers associated with NSAIDs" NEJM vol 338, number 11, March 12, 1998 pg 727.
OTHER USES FOR MY MATERIAL
©2004 All rights reserved. I would like to share my materials for educational purposes, but please don't alter the slides or animations (such as removing the author's signature) without letting me know. I would want to know about any commercial use.
As I have said above, I am very interested in sharing all the materials on my web site. The flash movies can be run as "Projectors" off computer hard drives or removable media, such as CDROMs, or data DVDs. The Projectors contain all the necessary drivers. The new Macromedia technology makes for high quality, but very compressed files and these materials take up little space. All of my three E-books can be placed on one CDROM.
Also, my content is scaleable, i.e., I would like to run my E-books off of institutional intranets. That way I can enlarge my animations by 2X or more, and use the highest quality setting (now the best quality is only at 90%. The 90% to 100% improvement increases file sizes by 4Xs!!!!!!). I believe the students will enjoy the format even more.
My ultimate goal is to encourage other educators to contribute to this type of learning tool. I can only see the possibilities getting better and better.
Lastly, all of this material can be rendered as 1920 by 1080 pixel resolution. It takes one of my big workstations about a week or two to do it, but she doesn't mind, she has nothing better to do, and I think she likes the work. My point is that some of this content is dazzling (I might be just a little bit biased) when run at that resolution on a large plasma screen monitor. So is there anyone who is interested in developing HDTV content? From what I've seen, they certainly need some more.
So contact me.
Craig Wiesenhutter.